The Safe Position in Immobilization
There is a specific position of safe immobilization for every joint that requires careful consideration. Immobilization in a different position can lead to contractures, stiffness, limited range of motion and inadequate healing.
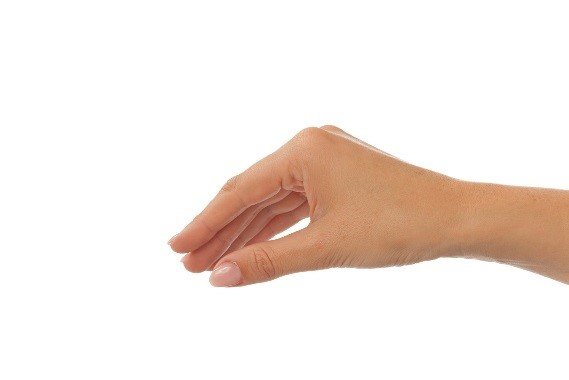
The overall safe position of immobilization for the hand is called the intrinsic plus or clam digger position. In the intrinsic plus position, the MCP joints are positioned in flexion and the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints of the fingers are positioned in extension.
This position takes into consideration:
- the joint structure
- the intrinsic muscles
- the collateral ligaments
Anatomical Review
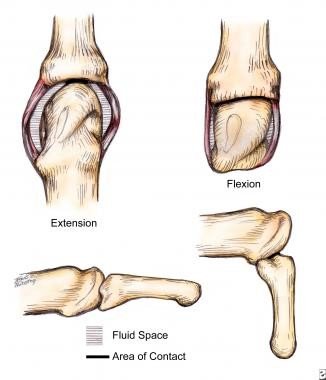
The metacarpal heads have an ovoid shape in the sagittal plane, and this widens from the dorsal to the volar dimension. The collateral ligaments are positioned dorsal to the axis of rotation of the MCP joint. This unique anatomy leads to a varying degree of tightness of the collateral ligaments based on the joint position. When the joint is in extension, the collateral ligaments are lax. In flexion, the collateral ligaments span a wider distance and are tight.
The MCP joint is curved in two planes to permit abduction, adduction, and rotation, as well as flexion and extension in an abbreviated ball-and-socket configuration. In flexion, the MCP joints are very stable and the bone surface area contact is greater than it is in extension.
The collateral ligaments of the proximal inter-phalangeal joint (PIP) originate close to the axis of rotation, providing a smaller change in length with changes in joint position, which provides lateral stability. The PIP joint ranges in only one plane, and its shape also adds to its lateral stability.
Source images: http://emedicine.medscape.com
-

-
The MCP Joint
-
-
The PIP Joint
The Intrinsic Muscles
The intrinsic muscles of the hand include the interossei (4 dorsal and 3 volar) and the lumbrical muscles. These muscles work together to flex the MCP joints and extend the PIP and distal inter-phalangeal (DIP) joints. The interossei also act to abduct and adduct the fingers.
The Volar Plates
There are some structural differences between the volar plates of the MCP and IP joints. The MCP volar plate is composed of many interlocking bands of fibres that collapse like an accordion on flexion and expand with extension.
The volar plates of the PIP and DIP joints are more rigid structures that do not collapse but glide with movement. They are attached to the proximal phalanx only by the proximal checkrein ligaments. Therefore, the rigid IP volar plate can glide a bit proximally and distally with joint motion which adds to the protection of the joint.
When injured
When the fingers get injured, oedema forms as the initial response. Joint stiffness may develop quickly as fluid accumulates within the joint spaces, and causes swelling of the joint capsules. Increased fluid content within the articular capsule and collateral ligaments effectively shortens these structures, favouring extension.
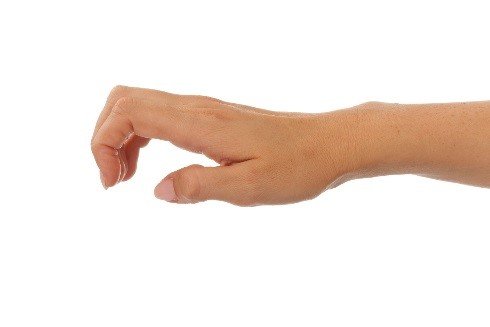
In extension, the MCP joint can accommodate this increased fluid content. As the MCP joints extend, the flexor tension on the IP joints increases and the extensor tension decreases. This causes the PIP and DIP joints to flex. Which may result in the intrinsic negative or minus hand, consisting of MCP joint extension, IP joint flexion, thumb adduction and wrist flexion.
Orthotic Management
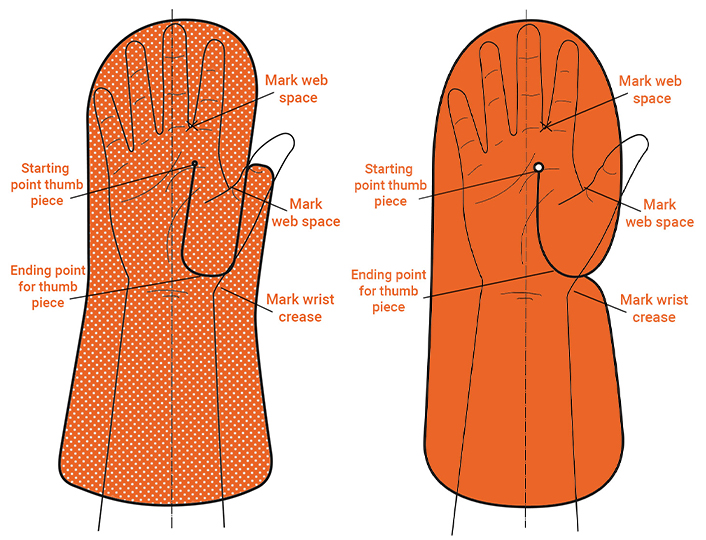
The best position in an orthosis for the injured hand with oedema is with the MCP joints positioned in flexion and the PIP and DIP joints positioned in extension.
The wrist should be in extension (20-30 degrees) and the thumb in wide abduction and slight IP flexion, in front of the index finger. If this position cannot be achieved initially, it is always possible to remould the orthosis with the reduction of oedema and range of motion gains.
-
-
Intrinsic Minus hand
-
-
Intrinsic Plus hand
-

-
Proper resting position in orthosis
We offer many different materials that work perfectly for resting hand orthoses in the safe intrinsic hand position. For an adult, 1/8” or 3.2 mm works best, but for smaller individuals and children, 1/12” or 2.4 mm – 2.5 mm may be appropriate.
Have a look at the following Splinting Guides for a quick tutorial of suitable resting hand orthoses:
Elastic Materials:
Orfit Classic
Orfit NS
Orfit Natural NS
High Resistance to Stretch (for larger limbs):
Orfit Eco
Orfit Eco Black NS
Orfibrace NS


Written by Debby Schwartz, OTD, OTR/L, CHT
Physical Rehabilitation Product and Educational Specialist at Orfit Industries America.
Debby is a certified hand therapist with over 36 years of clinical experience. She completed her Doctorate of Occupational Therapy at Rocky Mountain University of Health Professions in 2010. She has worked at Orfit Industries America as Product and Educational Specialist since 2007.
Debby is also an adjunct professor at the Occupational Therapy Department of Touro University, School of Health Sciences, and at the Occupational Therapy Department at Yeshiva University, Katz School of Science and Health in NYC. She has written many book chapters in the field of hand therapy and multiple articles for hand therapy journals, including the ASHT Times and the Journal of Hand Therapy. She has published a new textbook on orthotic fabrication together with Dr. Katherine Schofield, entitled “Orthotic Design and Fabrication for the Upper Extremity: A Practical Guide”.
Debby’s Google Scholar
Contact us for more product information or find your local distributor here.

If you’d like to receive the latest product updates and interesting Orfit news, subscribe to our newsletter:

