
Our Orfit blog shares information and instructions in matching our thermoplastic materials to orthotic designs.
Please check back frequently to gain inspiration and ideas in orthotic fabrication for all of your patient’s needs.
Splint Design: Lever System for Hemiplegia
Objective of the splint: Prevention of tissue shortening.

Pathology: Hemiplegia, spastic phase
One of the main problems we face with hemiplegia is tissue contractures. There are several causes, beginning with edema leading up to articular stiffness, and eventually muscle shortening.
The concerns are localized differently during each phase: during the flaccid phase, the concern is geared towards the level of the hand which we very often position flat, for example on a pillow. This is the reason why an orthosis that supports the hand in the intrinsic position can be useful during the night.
During the day, the dorsal wrist cock-up splint could be used to avoid wrist flexion. This design is better than the volar one because it preserves more sensitivity.
In the spastic phase, the concern shifts to the entire upper limb, from the elbow up to the fingers.
This is one of reasons why the Bobath association recommends the arm swinging during walking, eliminating the need of wearing a supportive sling.
A strictly volar orthotic design might not be the best solution in this case, because it can cause friction which could prevent the optimum articular positioning. Furthermore, there are risks of hyper pressure which can cause wounds or bedsores: the maximal amount of tissue compression at the fingertips, without risk of tissue damage, is 50g / cm2.
The lever system is a good solution because it is easier to don and doff the orthosis. Also biomechanically it is more interesting: if you provide a force of 100 grams on the proximal side of the extremity, you obtain approximately 200 grams of force at the distal part of the extremity (as the momentum is influenced by the distance from the center of rotation). In addition, there is no risk of friction on finger length either.
The splint pattern consists of two parts: the first pattern is for splinting the wrist and long fingers and the second one is an additional piece to position the thumb. But most of the time, you may be able to eliminate the additional material to position the thumb.
The thenar muscle is a key spot which can be used to inhibit spasticity as you can obtain excellent results providing pressure on it for example with a Velcro tape. You can stick the Velcro strap in front of the arch of the hand, which is located at the third MCP joint. Afterwards, orientate it toward the MC joint, base of the first metacarpal, as shown in the below picture:
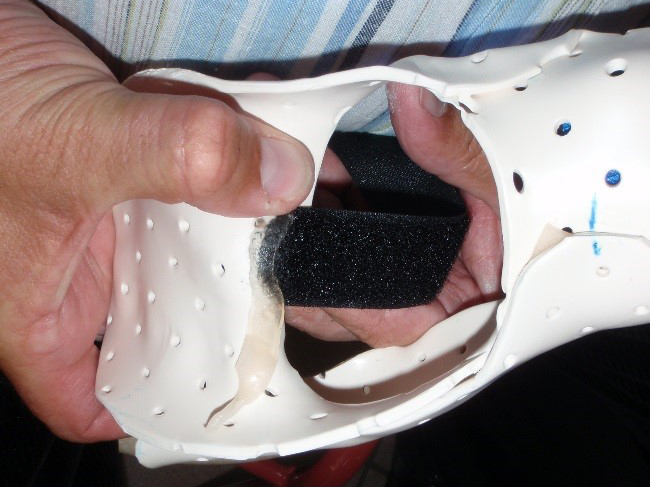
As you can see, the loop tape is securely fastened at the internal part of the orthosis. By using a small piece of very sticky thermoplastic (like Orfit Classic Soft 1.6 mm) you can make sure it will stay on permanently. Press it firmly together to prevent it from becoming a local pressure point. As an alternative, you can also use a piece of Orficast, which is thinner than regular splinting materials.


Product Recommendations
A non-elastic splinting material is highly recommended for this type of anti-spasticity orthoses to avoid fingerprinting. These materials will also stay in place while obtaining the correct position during molding.
Orfit Eco and Orfibrace are excellent choices. If you choose Orfit Eco Black NS or Orfibrace, you will have to scrape off the NS coating in order to attach the Velcro straps.
You can also use our Orfit Classic stiff precut (in sizes Small, Medium and Large), which eliminates the need to make a pattern. Instructions are provided in our online Educational Corner.
By adding a thumb piece, you will obtain this orthosis:
As it is recommended to provide pressure rather than to provide traction, the thumb piece is positioned externally and the Velcro strap will provide pressure on the thenar (first metacarpal) and onto the first and second thumb phalanges.
Try to position the extremity in the intrinsic position as much as possible, but avoid overcorrections as they might cause local pressure points (Zancolli scale).
Wearing protocol:
Typical wearing schedules for this type of orthosis are during the night.
If the patient wears it day and night, the risk of having a hemi-neglect syndrome will increase.
Daytime should be saved for rehabilitation and mobilization exercises.
Questions?
If you have a question or comment, please post it in the Orfit Splinting & Rehabilitation Group on Facebook, or send an email to welcome@orfit.com.


